The macular is the central and most important part of our retinas. It is responsible for our central vision which we use every moment of everyday of our waking lives. Our peripheral vision is important too but it is the central vision that we rely on to identify everyday objects, revealing the details of nature, looking at the letters on the vision chart, and recognising faces. Essentially it is the part that gives us our high-definition vision.
Our retinas are one of the most used parts of the body. The macular region works the hardest throughout the day. When light enters the eye, it is absorbed by photoreceptors in the retina which then triggers a complex sequence of chemical reactions. These chemical reactions are then passed along to the visual areas of the brain to be translated into ‘vision’. These chemical reactions expend a lot of energy and require a lot of maintenance.
We rely on the same retina and macular for our whole lifetimes. Unlike the rest of our body systems, we are unable to regenerate the cells of the retina. With the eyes being in constant use from the moment we open our eyes to the time we close them for sleep, it is not surprising that the ageing process affects the retina first and in particular, the macular.
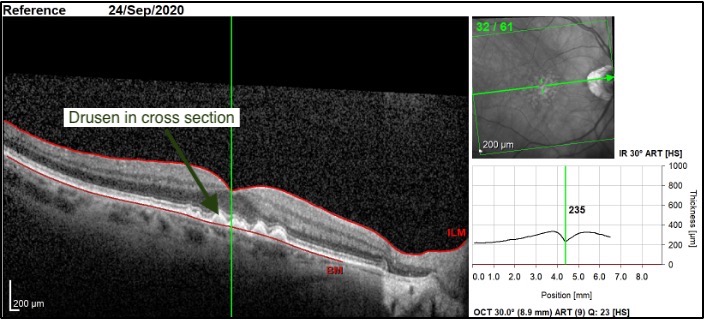
As there are no symptoms in the early stages of macular degeneration, it is important to have regular eye exams to identify disease early. Optical coherence tomography and fundus imaging are vital assessment techniques to detect and monitor signs of physical macular changes.
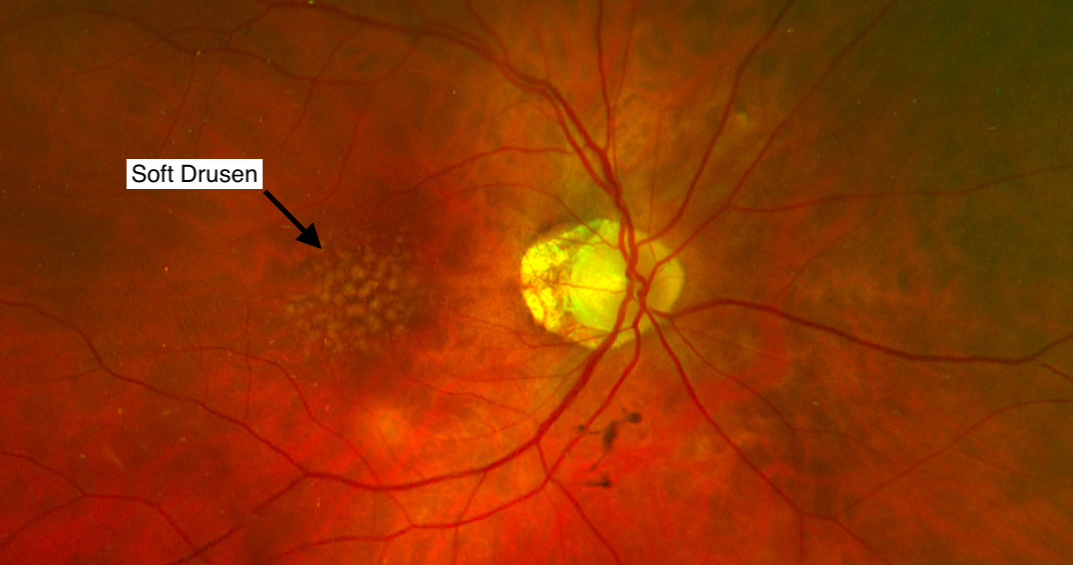
The first signs and symptoms of macular ageing include the development of drusen and retinal pigment changes. Normally the waste materials from the photoreceptor chemical reactions are removed from the retina. As the retina gets older, this process to slow and causes the waste products from this process to accumulate. This accumulation occurs between the retinal pigment epithelium and the choroid to form yellow spots called drusen.
In ‘Dry’ macular degeneration, shortened as dry AMD, (also called ‘atrophic’) the drusen builds up and accumulates to cause damage to the retina. As the degeneration advances, geographic atrophy develops leading to blind spots in the centre of vision. This is the most common form of macular degeneration, often occurring gradually, and is less severe.
‘Wet’ macular degeneration, shortened as wet AMD, (also called ‘exudative or neovascular’) can occur more suddenly and vision can be impaired rapidly potentially leading to vision loss. The ‘Wet’ change happens when there is a breakdown of a layer of the retina called Bruch’s membrane, causing blood vessels to breakthrough into the retina at the macular. These abnormal blood vessels can break and leak fluid causing the macular to become distorted. This process generally results in rapid loss of central vision unless detected early and treated early.
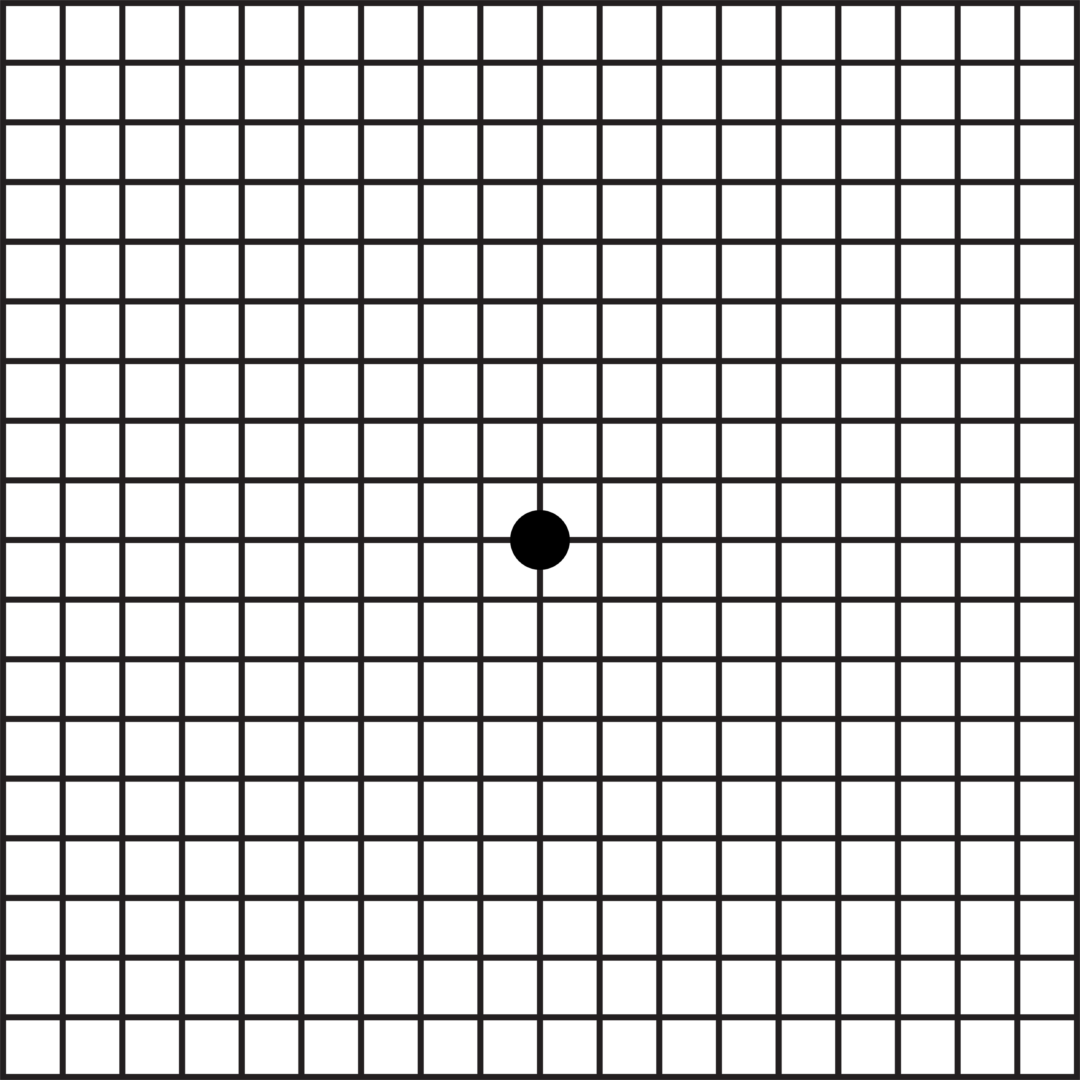
It is therefore important to self-monitor from time to time to check for early wet macular degeneration symptoms and signs. The Amsler chart is something you can use to detect early subtle effects to your vision. Click here to access the Amsler chart. Should there be concerns, it is important to also follow up your self monitoring with check ups from a professional.
Vision is not affected in the initial stages but as it progresses, one may start to notice changes to their central vision:


Whilst there is no macular degeneration cure, there are treatment options for both wet & dry AMD. The current treatment and options can help alleviate or even delay the condition.
This form of degeneration requires urgent treatment by a retinal specialist ophthalmologist or specialist retinal clinic. Historically, Wet AMD was treated with laser photocoagulation or photodynamic therapy (PDT).
The wet macular degeneration treatment currently recommended is anti-vascular endothelial growth factor (Anti-VEGF) injections. The drugs stop new abnormal blood vessels from forming and breaching the retina. The anti-VEGF injections are repeated on a regular basis until the neovascularisation process is stabilised.
Up until recently, there has been no clinically dry macular degeneration treatment available. Often, the recommended treatment has been based upon improving diet, taking macular supplements and smoking cessation programmes.
Exciting news is that there is now photodynamic therapy treatment available for dry age-related macular degeneration. The treatment is provided by a device called the Valeda Light Delivery System by Lumithera.